










 174 / 460
174 / 460

The history of the trochlear dysplasia in patella dislocation
173
crossings of the two condyles with the floor of
the trochlea and the condyles are asymmetrical,
Type III
is a severe form of trochlear dysplasia
where the condyles are symmetrical and the
crossing is situated low (distally) in the groove
(fig. 4).
H. Dejour and G. Walch also introduced two
quantitative criteria for trochlear dysplasia that
they were not integrated in this first
classification. The “trochlear bump” or
prominence represents the elevated trochlear
floor from the anterior distal femoral cortex
proximally to the crossing sign, and the
“trochlear depth” that measures the depth of the
trochlear floor from the condyles distally to the
crossing sign (fig. 5). A trochlear depth of 4mm
or less was found to be pathological [8]. The
importance of this radiographic analysis was
that for the first time trochlear dysplasia was
related to the reduced height of the lateral facet
(trochlear depth), the elevated trochlear floor
(prominence) or both. The impact of the work
of this group of surgeons was so great that for
many years, French surgeons were treating
patellofemoral instability based on these results
and consider patellar dislocation as a
multifactorial entity of imaging findings
surrounding trochlear dysplasia [10], a concept
that initially attracted a lot of interest and was
sometimes a field for overseas criticism. The
conclusions from these new findings about tro
chlear dysplasia and the trochlear prominence
led Henri Dejour to propose a new surgery for
the treatment of high-grade trochlear dysplasia.
He described a deepening trochleoplasty where
the bump was removed and the groove was
recreated by doing a osteotomy in the native
groove and then by fixing it with two screws
medially and laterally leading to compression
of both facets [8, 31, 33] (fig. 6) [28].
In 1994, the Swiss surgeon H. Bereiter
recommended a third operation for the
treatment of trochlear dysplasia [34]. This was
known as the “Bereiter” procedure [35]. In
2002, D. Goutallier performed the fourth type
of trochleoplasty procedure [36]. The first
results of the “recession-wedge” trochleoplasty
were published, and this technique was
embraced by P. Beaufils in Paris [37]. In 2010,
L. Blønd from Copenhagen presented his
innovative technique of Bereiter’s arthroscopic
trochleoplasty [38].
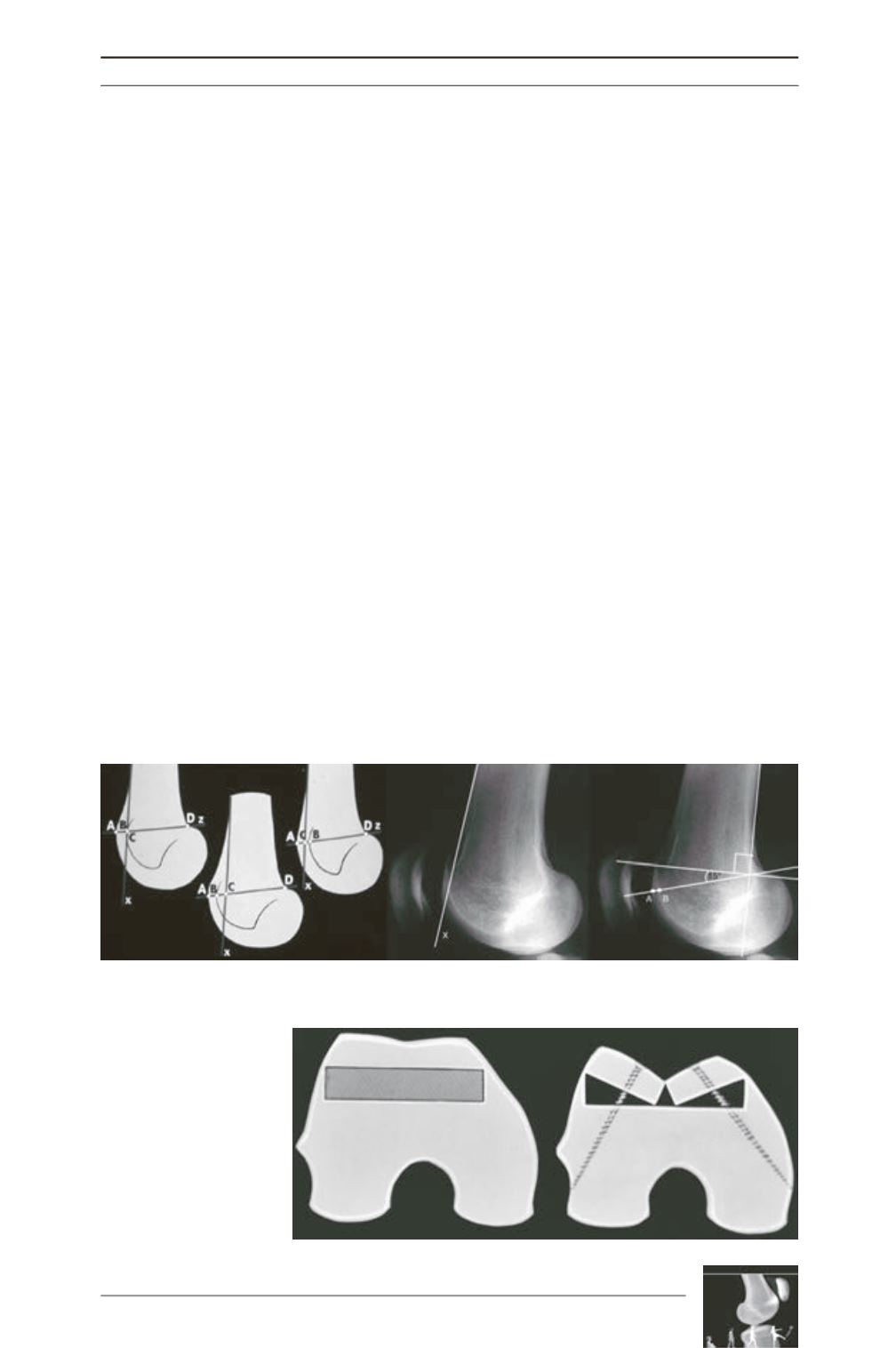
Fig. 5: (Original slide) The ‘trochlear bump’ or ‘prominence’ represents the elevated trochlear floor from the
anterior distal femoral cortex (distance A-B, left) proximally to the crossing sign, and the ‘trochlear depth’
(distance B-C, left) represents the depth of the trochlear floor from the condyles distally to the crossing sign.
Fig. 6: (Original slide) The
deepening trochleoplasty
proposed by H. Dejour.