










 202 / 460
202 / 460

Recession wedge trochleoplasty for major trochlear dysplasia
201
tibial tubercle offset from the trochlear groove
(TT-TG distance) [10], to assess severity of
trochlear dysplasia on the horizontal cuts
according to the Dejour system [11] (
grade A:
crossing sign and shallow trochlea;
grade B:
crossing sign, supratrochlear spur, flat trochlea;
grade C:
crossing sign, double contour (“double
shape”), asymmetry of trochlear facets;
grade
D
: grade B + C, asymmetry of trochlear facets,
and cliff pattern) and to measure PTA,
subtended on CT scans by a line from one
corner of the patella to the other and measured
as the deviation of this line from the posterior
femoral condyles.
Operative technique
The patient was positioned supine. The
procedure was carried out under tourniquet.
Approach was made just lateral to the patella,
across the tibial tubercle (TT), and more distally
along the anterior ridge of the tibia in order to
performTT transfer in the same step if required.
The technique aimed to treat the underlying
anatomical abnormality without compromising
the articular surface. This operation was
combined with proximal or distal realignment
to allow improved patellar tracking and limit
the risk of recurrence of patellar instability.
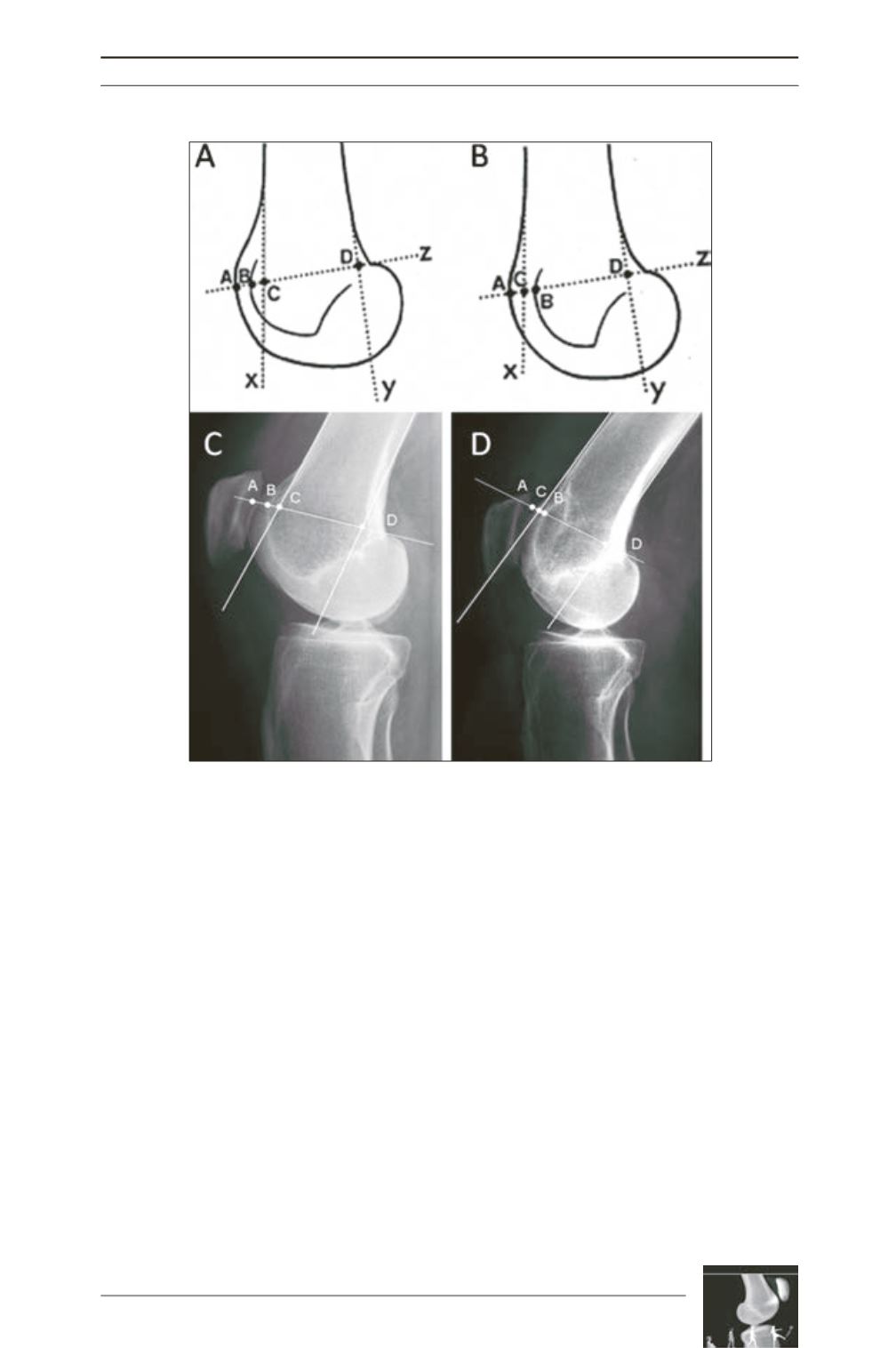
Fig. 2: Pre- and post-operative bump height measurement technique. 2A and 2B:
Drawings showing the Dejour and Walch method [7] for calculating bump height.
Point “D” is the junction between the posterior cortex and articular cartilage.
Bump height is measured between points ‘‘B’’ and ‘‘C”. 2C: Pre-operative lateral
radiograph: the bump height is positive. 2D: Postoperative lateral radiograph: the
bump height is now negative.