








 29 / 242
29 / 242

Place of navigation in 2014: why I resolutely navigate all my TKA?
29
Navigation modified also my way of thinking
when regarding the rotation of the femoral
implant. Currently, I externally rotate the
femoral implant in only 10% of the cases and
even I do not hesitate to internally rotate the
implant in 2% of the cases. External rotation is
given when the FMA is in valgus (above 3° of
valgus) and when the flexion gap is tight on the
medial side or lax on the lateral side. Internal
rotation is given when the FMA is in varus
(above 3° of varus) and when the flexion gap is
lax on the medial side. In the other cases, the
femoral prosthesis is implanted parallel to the
posterior bicondylar line with no additional
rotation.
Finally, navigation is very interesting to
evaluate the sagittal balance of the knee that is
flexum or recurvatum, which is not so easy to
measure before and after the implantation of
the prosthesis with a conventional procedure.
In these cases, navigation allows to cut less or
more bone of the distal part of the femur in
order to fit exactly the prosthesis to the
extension gap and to avoid toomuch recurvatum
or flexum.
Why I resolutely
navigate allmy TKA?
Considering everything I’ve learned in
17 years, it seems difficult to do TKA without
navigation. The best indications to use
navigation are severe deformities (fig. 2, 3,
4, 5), malunions of the tibia or the femur [16,
17] (fig. 6, 7, 8, 9 10) and when there is
unremovable femoral hardware [16, 18]
(fig. 10, 11, 12). However these indications are
not so frequent and if one only uses navigation
for these rare cases, the procedure will be very
boring and time consuming for the surgeon and
his entourage. We do well what we do often!
Conclusion
Currently, Computer-assistedTKAis performed
routinely in my department as well as
osteotomies of the knee, UniKA and UniKA
revisions. All the staff of the operative room is
well aware of the functioning of the device and
no time is lost around the operation. It is not
harder to manage than an arthroscopy of the
knee. There is no preoperative constraint to the
surgeon or his team and all decisions are taken
intraoperatively. Despite this fact, the procedure
takes only 5 to 10 minutes more that is
negligible, compared to all the benefits.
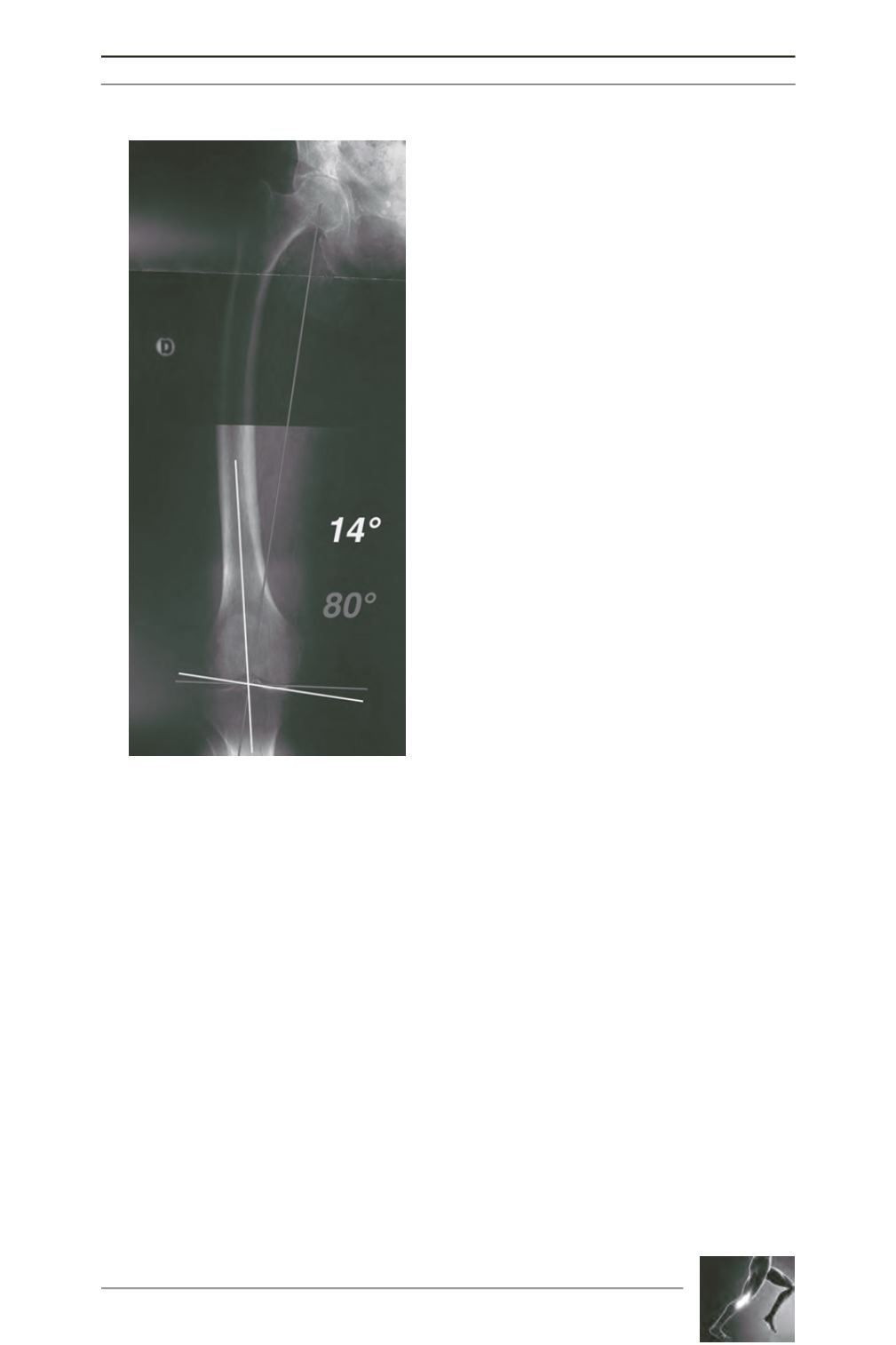
Fig. 1: Severe varus deformity of the femur.
The medial FMA is at 80°, that is 10° of
varus. It is impossible to put the femoral
implant at 90° with a conventional ancillary
without tricking with the intra medullary
rod… It is very easy with navigation…