










 43 / 244
43 / 244

B. BORDET, J. BORNE, A. PONSOT, P.F. CHAILLOT, O. FANTINO
42
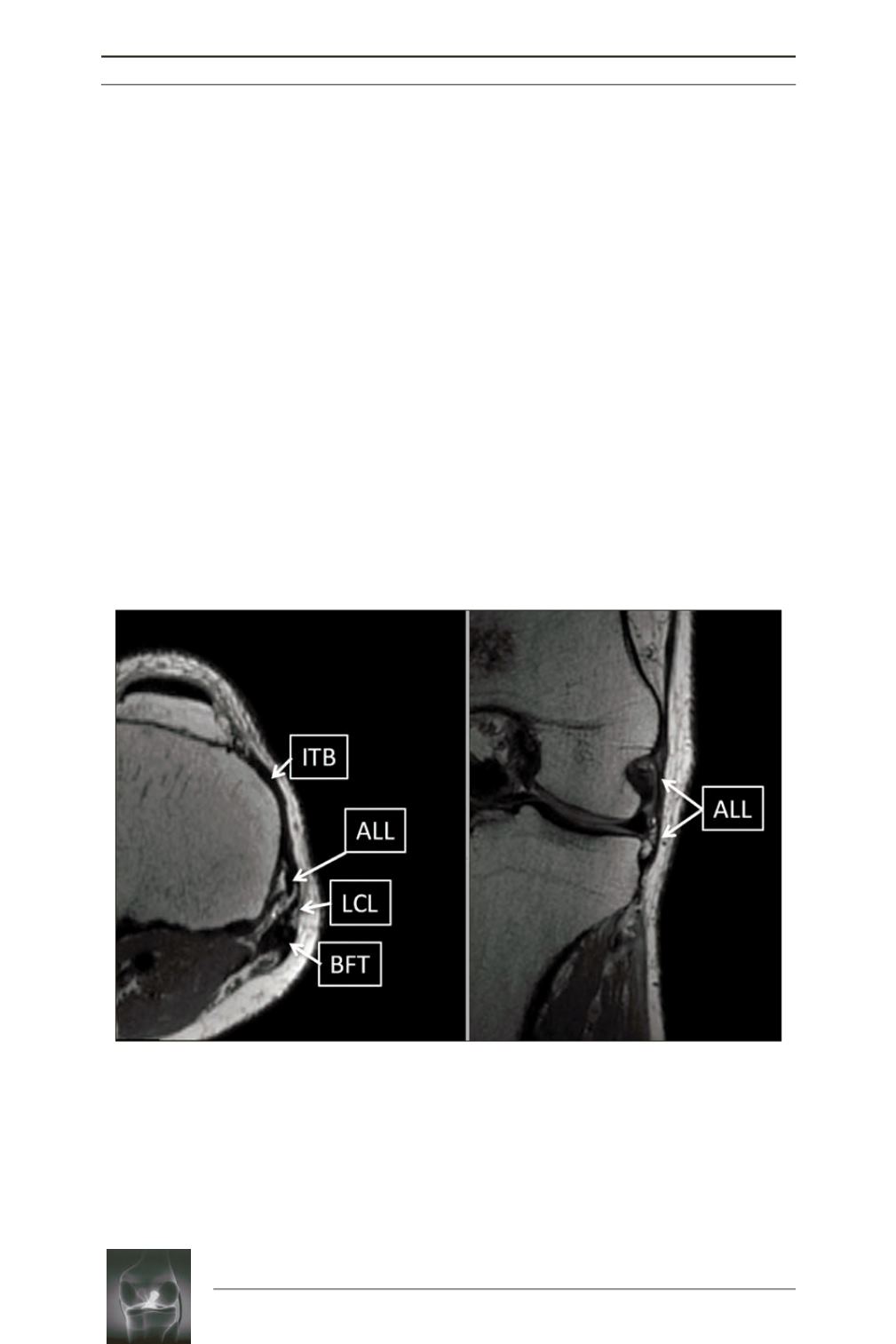
visible, in contact with the wall of the lateral
meniscus and the meniscal ligament expansions
can be studied [2, 3] (fig. 2).
Several projects are underway to study the
ALL in cases of ACL injury. Helito has shown
an injury in 30% of cases but these injuries are
predominantly proximal [4].
To date, two ultrasonography studies have
described the ALL [5, 6]. Mary Faruch
et al.
’s
study correlated ultrasonographic data and cada
veric dissections. A recent Japanese study using
real time virtual sonography showed that the
ligament was identified in 100% of cases [7].
In our experience [8] it is possible to explore
the ALL by ultrasound using high frequency
waves.
We study the ligament in a resting position with
the knee bent at 20° and we perform dynamic
flexion and double rotation maneuvers to tense
it in an internal knee rotation.
In a resting position, we clearly see this small,
relaxed, curved fibrillar structure that crosses
the lateral inferior genicular artery (LIGA),
located deeper, in contact with the lateral
meniscal wall. Above, we can see the thin
ligament that crosses the surface of the LCL.
Its femoral enthesis is more difficult to
distinguish due to a large insertion very close
to that of the LCL (fig. 3).
The dynamic maneuvers make the ligament
tense by flexion and internal rotation, with the
ligament approaching the lateral aspect of the
tibial plateau and straightening (fig. 4).
Fig. 2:
MRI of the ALL. 3D 1 mm-section MRIs, T2-weighted images. Axial and coronal multiplanar
reconstructions.
ALL
: anterolateral ligament,
ITB
: iliotibial band,
LCL
: lateral collateral ligament,
BFT
:
biceps femoris tendon.