










 63 / 244
63 / 244

A. SONI, V. MUSAHL
62
band changes it role from being an extender to a
flexor of the knee and will visibly reduce any
subluxation. Clinically, the magnitude of the
pivot shift is graded in accordance with the
subjective feel of the reduction as the anteriorly
subluxed tibia reduces. This subluxation/
reduction event occurs in the lateral compartment
at approximately 20-30 degrees of flexion. It is
always important to compare the exam to the
contralateral knee to determine if the patient
may have some underlying laxity when
performing this test.
COMING UPWITH A
STANDARDIZED MANEUVER
Differences in the amount of anterior tibial
subluxation during pivot shift testing have been
shown to vary considerably between examiners
[5], which may complicate the assessment of
this maneuver. These differences likely reflect
differences in the applied axial, valgus, and
rotational forces, as well as differences in the
position of the leg and knee flexion during the
maneuver. These subtle differences are further
amplified by variation in grading between
examiners for the same degree of subluxation.
Various systems of grading the pivot shift have
been recommended to allow for more uniform
evaluation of rotatory laxity.
To bring uniformity to the testing technique
and possibly decrease the effect of some of
above-mentioned variables, we described a
standardized pivot shift test maneuver [6]. It
was designed on the basis of Galway and
MacIntosh flexion type procedure [1]. Its
applicability was tested on 12 world renowned,
high volume ACL surgeons. Quantitative
results of their preferred pivot shift test
technique was compared to standardized
testing maneuver. It was found that the
variation of acceleration during the pivot shift
test across different surgeons utilizing their
preferred technique was significantly reduced
by performing the pivot shift test in a
standardized maneuver.
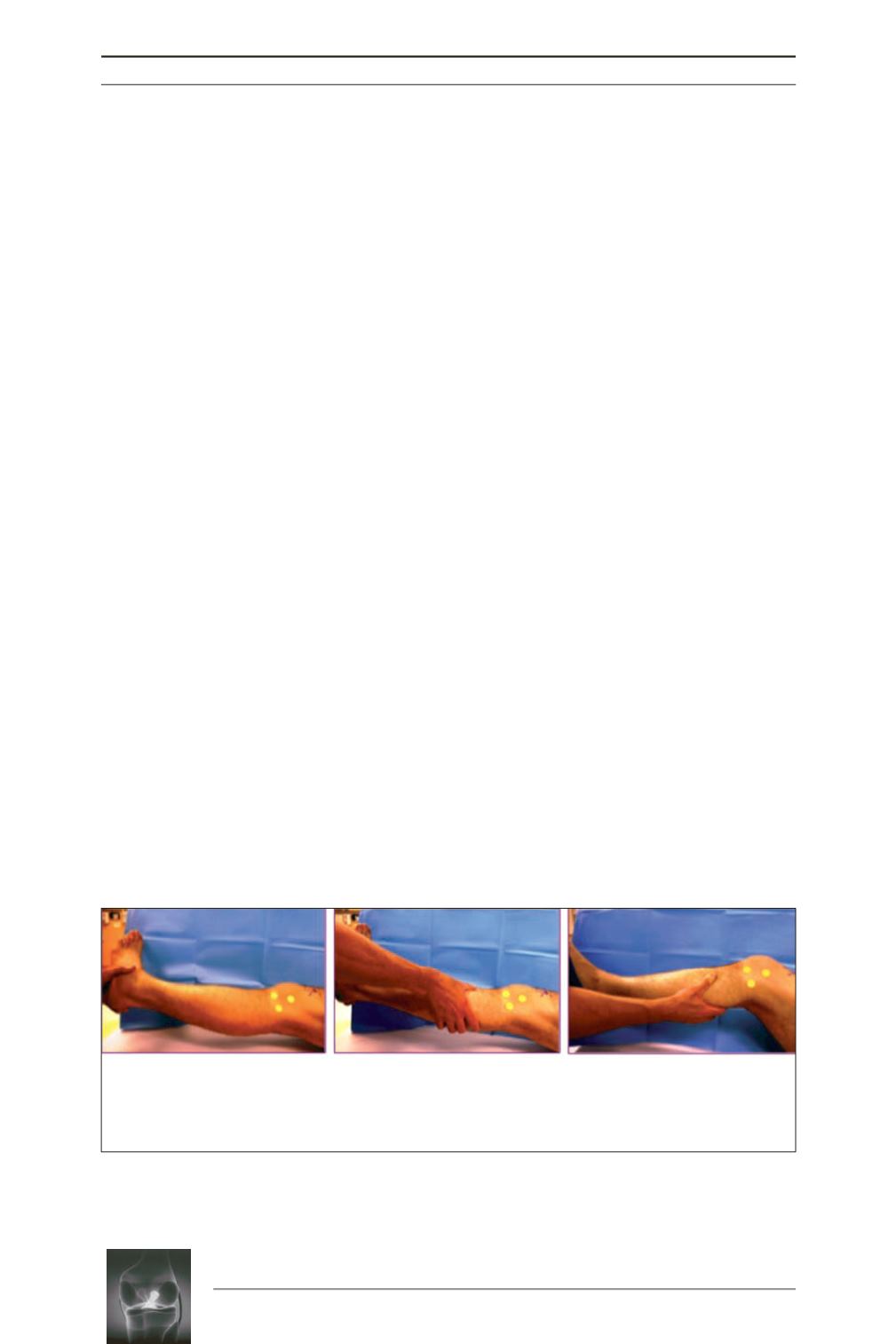
To assess left knee, the steps for this
standardized maneuver are as follows (fig. 1).
Step 1:
Stand facing the patient at foot level
and hold the heel with left hand. Abduct the hip
followed by internally rotating with left hand.
Step 2:
Put right hand with thumb up just distal
to joint line and apply gentle valgus stress, thus
allowing spontaneous flexion.
Step 3:
Flex the knee with the right hand and
release the rotational stress. Reduction
movement can be felt with the right.
Fig. 1:
Standardized maneuver in three steps.
Step 1:
Internal rotation
Step 2:
Valgus Stress
Step 3:
Flexion & Release
of Internal Rotation
1
2
3