










 211 / 460
211 / 460

P.R.F. Saggin, P.G. Ntagiopoulos, P. Ferrua, D. Dejour
210
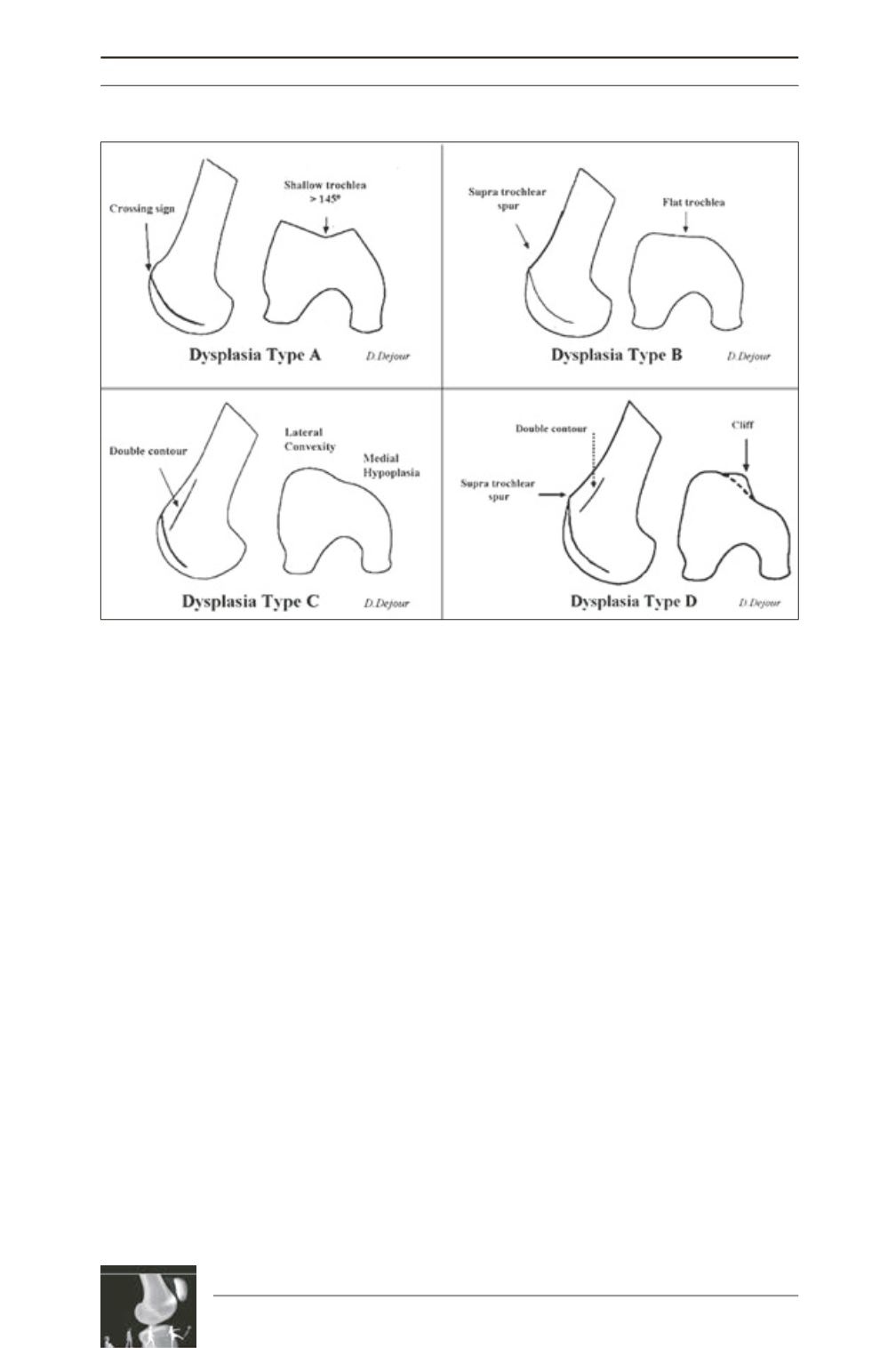
Trochleoplasty is indicated in dysplasia types
B and D, when there is prominence of the
trochlea. TypeAis lowgrade trochlear dysplasia
and should not be responsible for instability, if
present. Type C represents a subtype of
trochlear dysplasia not suited for sulcus
deepening trochleoplasty since the trochlea is
already hypoplastic and bone removal is
contraindicated.
Open growth plates are a contraindication to
trochleoplasty. Early (or established) arthritis is
another contraindication since trochleoplasty
can worsen the cartilage status.
To achieve successful outcomes, associated
abnormalities should also be addressed. TT-TG
is corrected when trochleoplasty is carried out
since the trochlear groove is moved laterally
from its native location.
Surgical Technique
Positioning
The patient is positioned lying supine. A lateral
pad applied to the proximal thigh and a distal
support under the foot allow the knee to be kept
flexed by approximately 80 degrees. Full range
of motion is possible during the procedure.
Exposure
A straight midline incision is performed from
the superior patellar limit to the tibiofemoral
articulation with the knee flexed. The
arthrotomy is performed through the medial
capsule. Proximally, the
vastus medialis
obliquus
is split in line with its fibers 4cm
Fig. 1 : Trochlear dysplasia classification (D. Dejour).